")
Bilateral Polycystic Ovaries: Causes, Symptoms, Diagnosis & Treatment Options
A comprehensive, expert-reviewed guide to understanding bilateral polycystic ovaries — what your ultrasound report means, when to worry, and how to manage it effectively.
If your ultrasound report mentions "bilateral polycystic ovaries", you are probably feeling anxious about what it means for your health and your ability to have children. You are not alone — this is one of the most common findings in reproductive-age women, affecting roughly 1 in 5 women globally. The good news is that bilateral polycystic ovaries are highly manageable with the right medical guidance, lifestyle changes, and treatment plan.
In this comprehensive guide, our gynaecology experts at Arka Anugraha Hospital, Bangalore explain everything you need to know — from what this condition actually means, to how it differs from PCOS, the symptoms you should watch for, diagnostic criteria, treatment options, fertility impact, and even the cost of care in Bangalore.
What Does Bilateral Polycystic Ovaries Mean?
Let us break down the medical term so it is easy to understand:
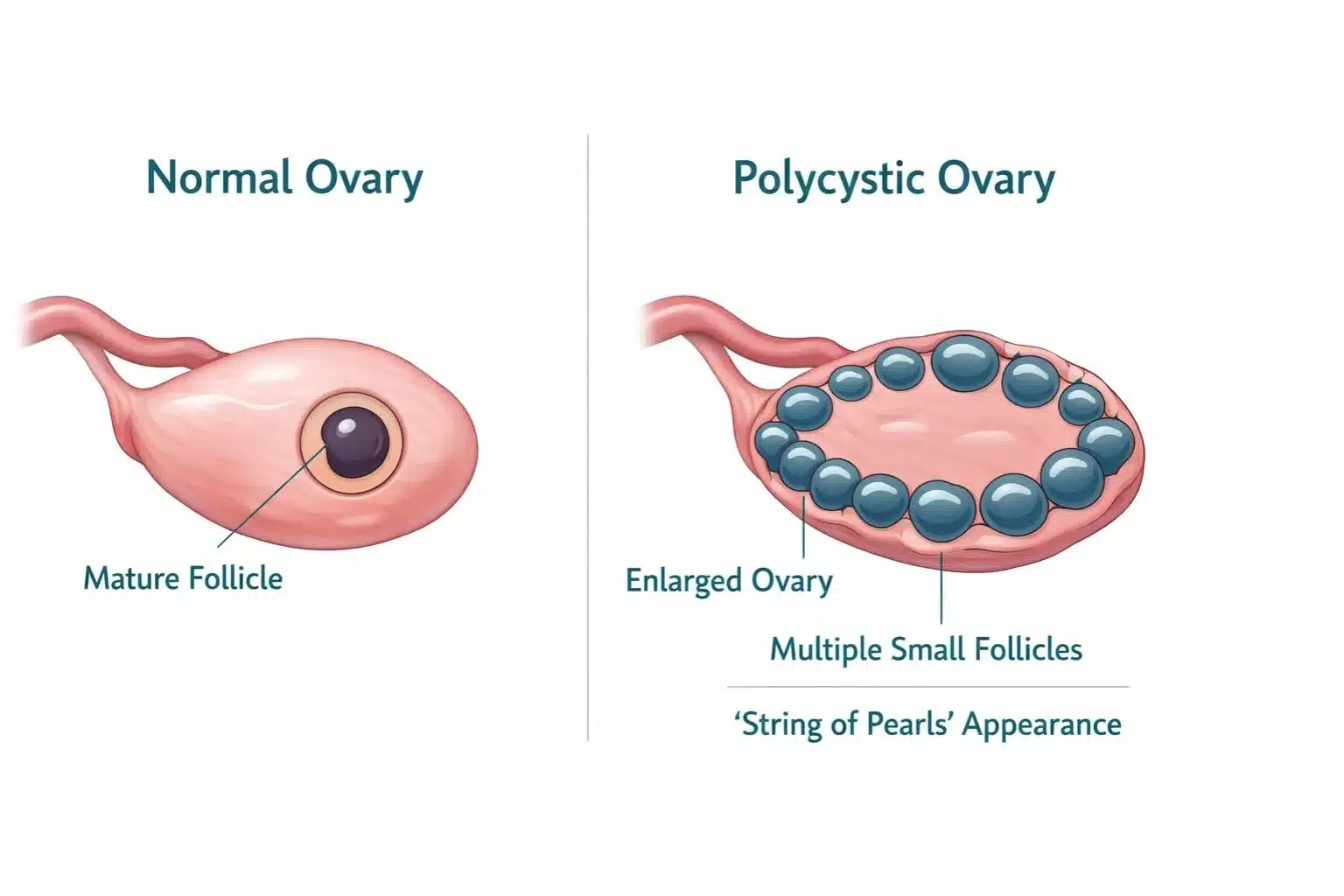
When a doctor says you have bilateral polycystic ovaries, it means your ultrasound scan has revealed 12 or more small follicles (measuring 2–9 mm in diameter) in each ovary, and/or your ovarian volume is greater than 10 ml. These follicles are immature eggs that have not been released during ovulation. On an ultrasound, they often appear arranged around the edge of the ovary, described as a "string of pearls" pattern.
Many women have polycystic-appearing ovaries without any hormonal problems or symptoms. It only becomes a concern when combined with other signs like irregular periods or elevated androgen levels.
Related Terms You May See on Your Report
Bilateral Bulky Ovaries: This means both ovaries appear enlarged — typically 1.5 to 3 times larger than normal size (normal ovarian volume is around 6–8 ml). The enlargement is caused by the accumulation of multiple small follicles.
Bilateral Polycystic Ovarian Morphology (PCOM): This is the clinical term used by radiologists to describe the ultrasound appearance of polycystic ovaries. It is one of the three criteria used in the Rotterdam diagnostic guidelines for PCOS.
Bilateral PCOD (Polycystic Ovarian Disease): This older term is often used interchangeably with PCOS in India. It refers to a condition where both ovaries are affected by hormonal imbalances and multiple cysts.
Bilateral Polycystic Ovaries vs. PCOS — What Is the Difference?
This is one of the most common sources of confusion. Many women assume that having polycystic ovaries on ultrasound automatically means they have PCOS. That is not always the case.
| Feature | Bilateral Polycystic Ovaries | PCOS (Syndrome) |
|---|---|---|
| What it is | An ultrasound finding | A hormonal disorder (syndrome) |
| Diagnosis | Ultrasound alone | Rotterdam Criteria (2 of 3 features) |
| Hormonal imbalance | May or may not be present | Usually present (elevated androgens) |
| Irregular periods | May be normal | Common (oligo/anovulation) |
| Fertility impact | Usually minimal alone | Can significantly affect fertility |
| Treatment needed | Only if symptomatic | Yes — lifestyle + medical management |
According to the Rotterdam Criteria (the international gold standard), PCOS is diagnosed when at least 2 out of 3 features are present: polycystic ovary morphology on ultrasound, irregular or absent ovulation (oligo/anovulation), and clinical or biochemical signs of elevated androgens (such as excess body hair, acne, or high testosterone levels on blood tests).
So, you can have bilateral polycystic ovaries without having PCOS. However, it is important to follow up with your doctor to rule out the syndrome, especially if you have any accompanying symptoms.
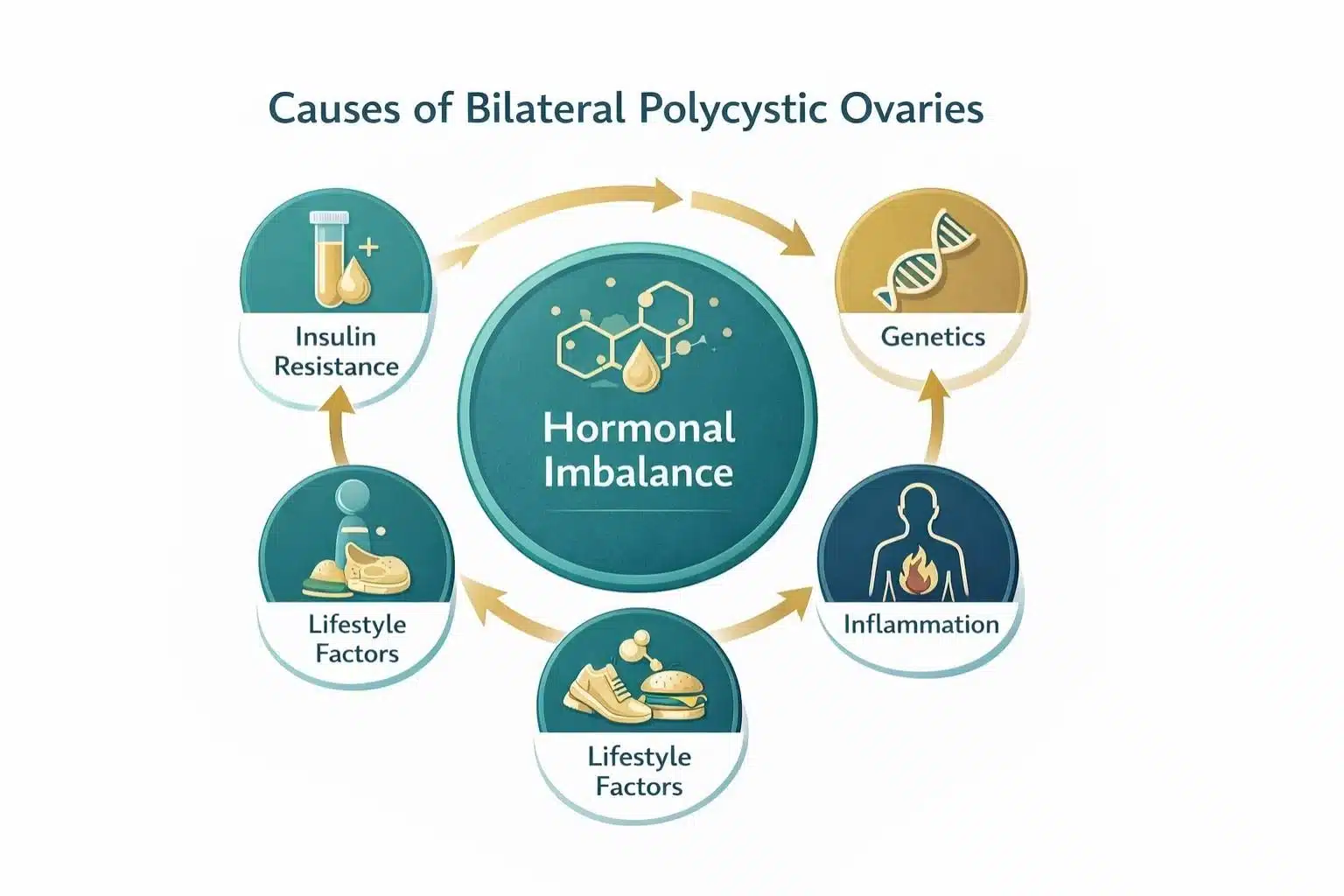
What Causes Bilateral Polycystic Ovaries?
The exact cause of bilateral polycystic ovaries is not fully understood, but research points to several contributing factors that often work together:
1. Hormonal Imbalance
Elevated levels of androgens (often called "male hormones," though women produce them naturally in smaller amounts) interfere with normal follicle development. Instead of one follicle maturing and releasing an egg each month, multiple follicles begin to develop but none mature fully — resulting in the characteristic polycystic appearance on ultrasound.
2. Insulin Resistance
This is one of the most significant underlying factors. When your body's cells become resistant to insulin, the pancreas produces more insulin to compensate. High insulin levels then signal the ovaries to produce excess androgens, creating a vicious cycle. Research suggests that up to 70% of women with PCOS have some degree of insulin resistance, regardless of their body weight.
3. Genetic Predisposition
If your mother, sister, or close female relatives have PCOS or polycystic ovaries, your risk is significantly higher. Multiple genes related to hormone production, insulin regulation, and inflammation have been identified as contributors.
4. Chronic Low-Grade Inflammation
Studies show that women with polycystic ovaries often have elevated markers of inflammation (such as CRP). This low-grade inflammation can stimulate the ovaries to produce more androgens.
5. Lifestyle Factors
While lifestyle factors do not directly cause bilateral polycystic ovaries, they can significantly worsen the condition. Obesity, sedentary lifestyle, poor diet (especially high in refined carbohydrates and sugar), stress, and irregular sleep patterns all contribute to insulin resistance and hormonal imbalance.
Symptoms of Bilateral Polycystic Ovaries
Symptoms can range from mild to severe and vary greatly from one woman to another. Some women with bilateral polycystic ovaries may have no symptoms at all, while others experience multiple issues that affect their daily life. Here are the most common signs to watch for:
Irregular or Missed Periods
Menstrual cycles longer than 35 days, fewer than 8 periods per year, or complete absence of periods (amenorrhoea). This is the most common symptom.
Excess Hair Growth (Hirsutism)
Unwanted hair growth on the face, chin, chest, back, or abdomen due to elevated androgen levels. Affects approximately 70% of women with PCOS.
Weight Gain
Particularly around the abdomen (central obesity). Difficulty losing weight despite diet and exercise. Linked to insulin resistance.
Acne & Oily Skin
Persistent, hormonal acne that does not respond to typical skin treatments, especially along the jawline and chin. Caused by excess androgen stimulation.
Thinning Hair on Scalp
Male-pattern hair loss (thinning at the crown or widening part) due to elevated androgens. Also called androgenic alopecia.
Skin Darkening
Dark, velvety patches on the neck, groin, or under breasts (acanthosis nigricans). This is a strong indicator of insulin resistance.
Difficulty Conceiving
Irregular ovulation makes it challenging to predict fertile windows and conceive naturally. This is one of the leading causes of anovulatory infertility.
Mood Changes
Anxiety, depression, and mood swings are common due to hormonal fluctuations and the emotional impact of visible symptoms.
Consult a gynaecologist if you experience any of these: periods that are absent for more than 3 months, extremely heavy bleeding, sudden rapid weight gain, difficulty getting pregnant after 12 months of trying, or visible physical changes like excess facial hair or severe acne.
How Are Bilateral Polycystic Ovaries Diagnosed?
A thorough diagnosis involves multiple steps to distinguish between polycystic ovaries (the ultrasound finding) and PCOS (the syndrome). At Arka Anugraha Hospital's OBG department, we follow a comprehensive diagnostic protocol:
Detailed Medical History
Your doctor will review your menstrual cycle patterns, weight changes, family history of PCOS or diabetes, skin and hair changes, and any fertility concerns. This helps identify the pattern and severity of your condition.
Physical Examination
A clinical assessment to check for signs of excess androgen (hirsutism, acne), acanthosis nigricans (dark skin patches indicating insulin resistance), BMI measurement, and blood pressure check.
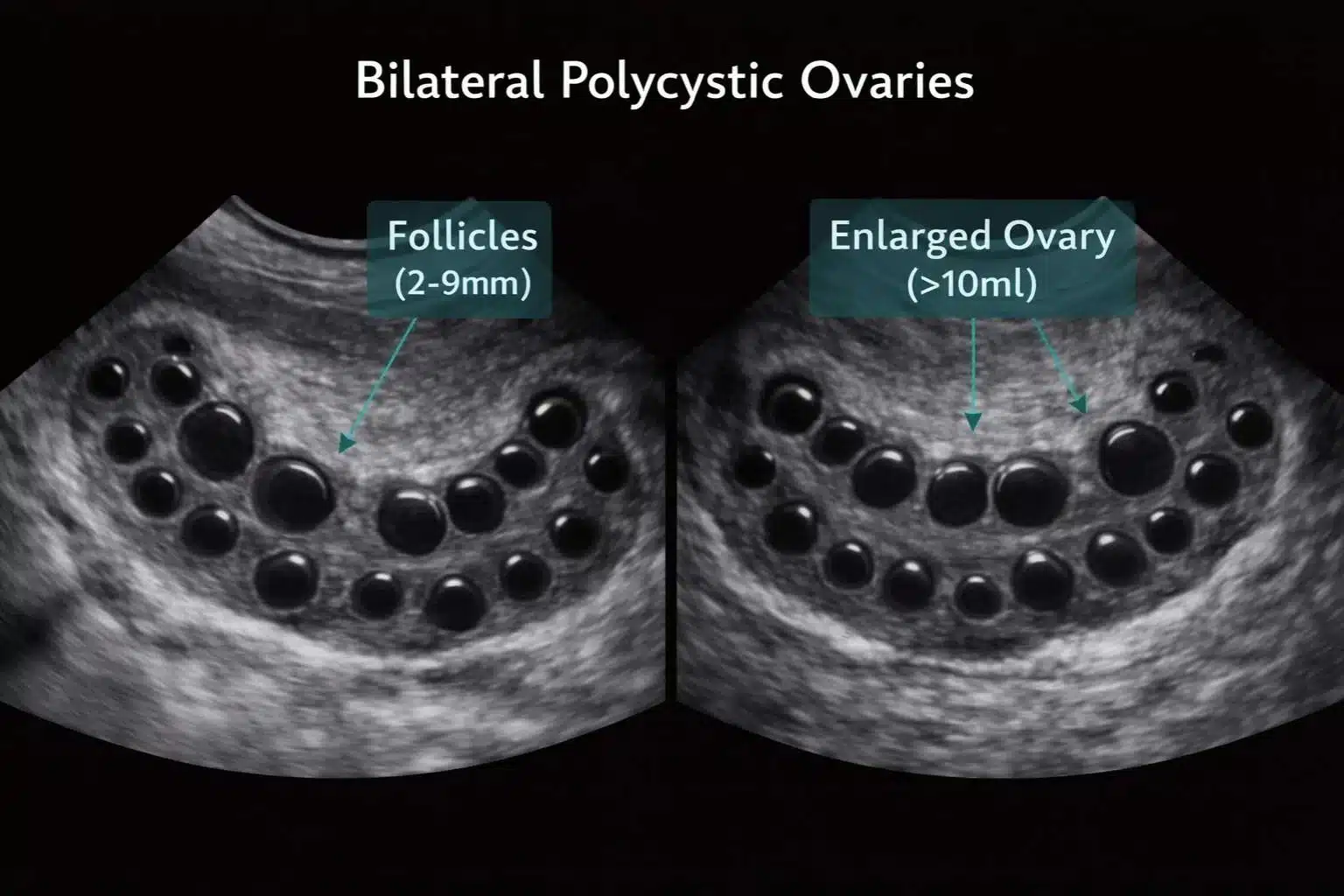
Pelvic Ultrasound (Transvaginal or Transabdominal)
The key diagnostic test. It reveals the number and size of follicles in each ovary, ovarian volume, and the arrangement of follicles. Bilateral polycystic ovaries are confirmed when 12+ follicles (2–9 mm) are visible in each ovary or ovarian volume exceeds 10 ml.
Hormonal Blood Tests
Measuring key hormones: LH (Luteinizing Hormone), FSH (Follicle-Stimulating Hormone), testosterone, DHEA-S, prolactin, and thyroid function tests (TSH, T3, T4). An elevated LH:FSH ratio (>2:1) is a classic finding.
Metabolic Screening
Fasting blood glucose, fasting insulin, HbA1c, and lipid profile to assess insulin resistance and metabolic syndrome risk. This step is crucial for long-term health management.
Is Bilateral Polycystic Ovaries Dangerous?
Bilateral polycystic ovaries by themselves are not dangerous. However, when they are part of PCOS and left untreated for years, they can increase your risk for several serious health conditions.
Short-Term Concerns
Irregular periods making planning difficult, fertility challenges due to irregular ovulation, cosmetic concerns like acne, excess hair, and weight gain that affect self-confidence, and mood-related issues such as anxiety and depression.
Long-Term Risks If Untreated
Type 2 Diabetes: Up to 50% of women with PCOS develop type 2 diabetes or prediabetes by age 40, especially those with insulin resistance.
Cardiovascular Disease: Metabolic syndrome (high blood pressure, abnormal cholesterol, high blood sugar) increases heart disease risk.
Endometrial Cancer: Prolonged absence of periods means the uterine lining is not being shed regularly, which can lead to endometrial hyperplasia and, in rare cases, endometrial cancer.
Obstructive Sleep Apnoea: Particularly in overweight women with PCOS.
Non-Alcoholic Fatty Liver Disease: Associated with insulin resistance and metabolic syndrome.
All of these long-term risks are significantly reduced with proper management. Lifestyle modifications like losing 5–10% of body weight, regular exercise, a healthy diet, and appropriate medication can dramatically improve your hormonal profile and metabolic health.
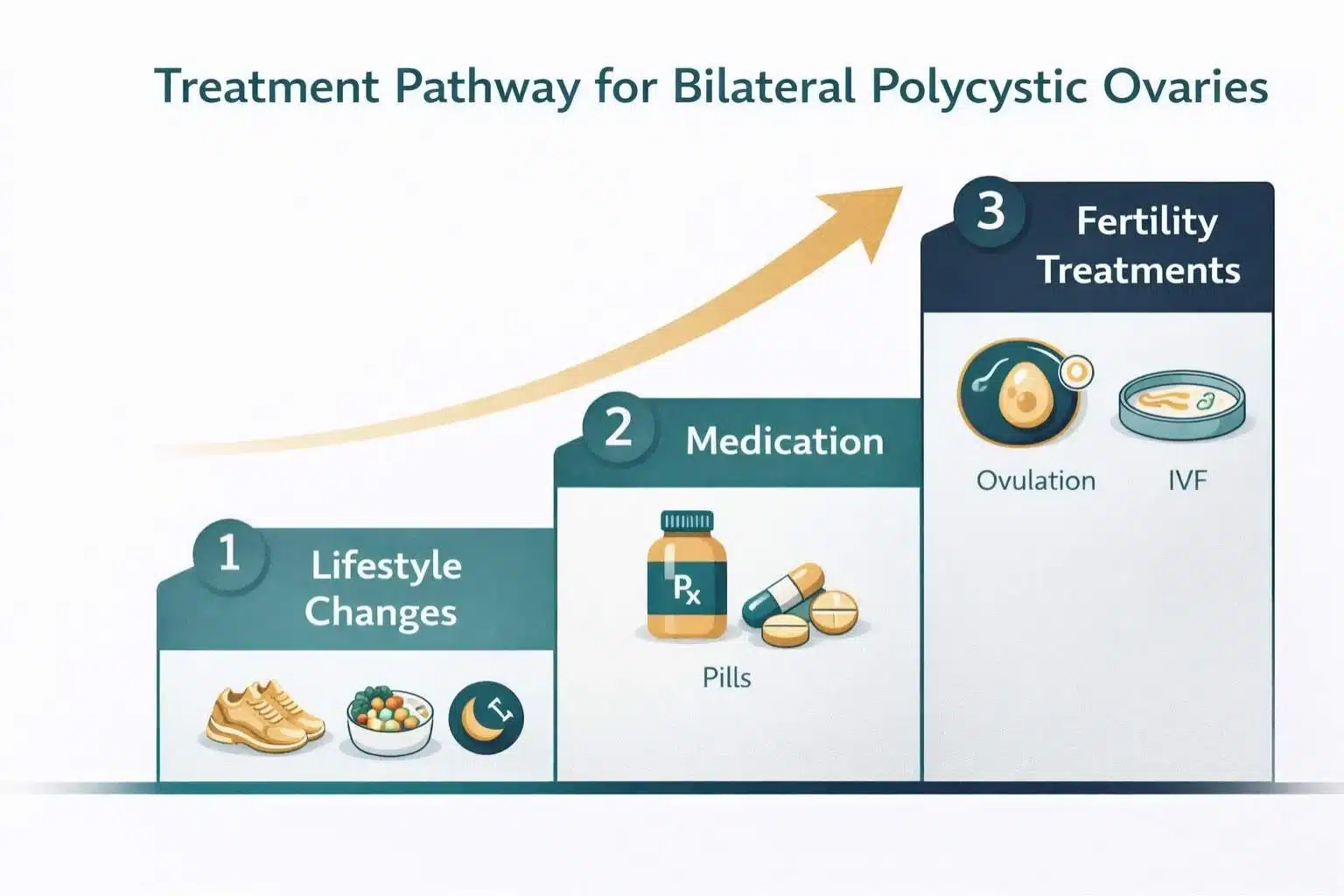
Treatment Options for Bilateral Polycystic Ovaries
Treatment is personalised based on your specific symptoms, whether you are trying to conceive, your metabolic health, and your overall goals. At Arka Anugraha Hospital, we follow a stepped approach:
Step 1: Lifestyle Modifications (First-Line Treatment)
This is the most important and effective intervention for the majority of women with bilateral polycystic ovaries. Research consistently shows that losing just 5–10% of body weight can restore regular ovulation, reduce androgen levels, improve insulin sensitivity, and lower cardiovascular risk. Focus areas include regular physical activity (150 minutes per week of moderate-intensity exercise), a balanced low-glycemic index diet, stress management (yoga, meditation), and adequate sleep (7–8 hours per night).
Step 2: Medications
For irregular periods: Combined oral contraceptive pills (COCs) containing oestrogen and progestin help regulate menstrual cycles, reduce androgen levels, protect the endometrium, and improve acne and hirsutism.
For insulin resistance: Metformin is commonly prescribed to improve insulin sensitivity, lower insulin levels, and help with weight management. It can also help restore regular ovulation in some women.
For excess hair and acne: Anti-androgen medications such as spironolactone can reduce hirsutism and acne. These are typically used in combination with contraceptive pills.
Step 3: Fertility Treatments (When Trying to Conceive)
Ovulation induction: Letrozole (preferred first-line) or clomiphene citrate are medications that stimulate the ovaries to release eggs. Letrozole has shown higher success rates and lower multiple pregnancy risks compared to clomiphene.
Gonadotropin injections: If oral medications do not work, injectable hormones (FSH) can be used under careful monitoring.
Laparoscopic ovarian drilling (LOD): A minimally invasive surgical procedure where small holes are made in the ovary using laser or heat. This can reduce androgen production and restore ovulation. Learn more about laparoscopic procedures at Arka Anugraha.
IUI and IVF: Intrauterine insemination or in-vitro fertilisation may be recommended when other treatments have not been successful. Explore our infertility services.
Dr. Saraswati Ramesh
Best Diet and Lifestyle Changes for Bilateral Polycystic Ovaries
Diet and lifestyle play a crucial role in managing bilateral polycystic ovaries. Here is an evidence-based approach recommended by our specialists:
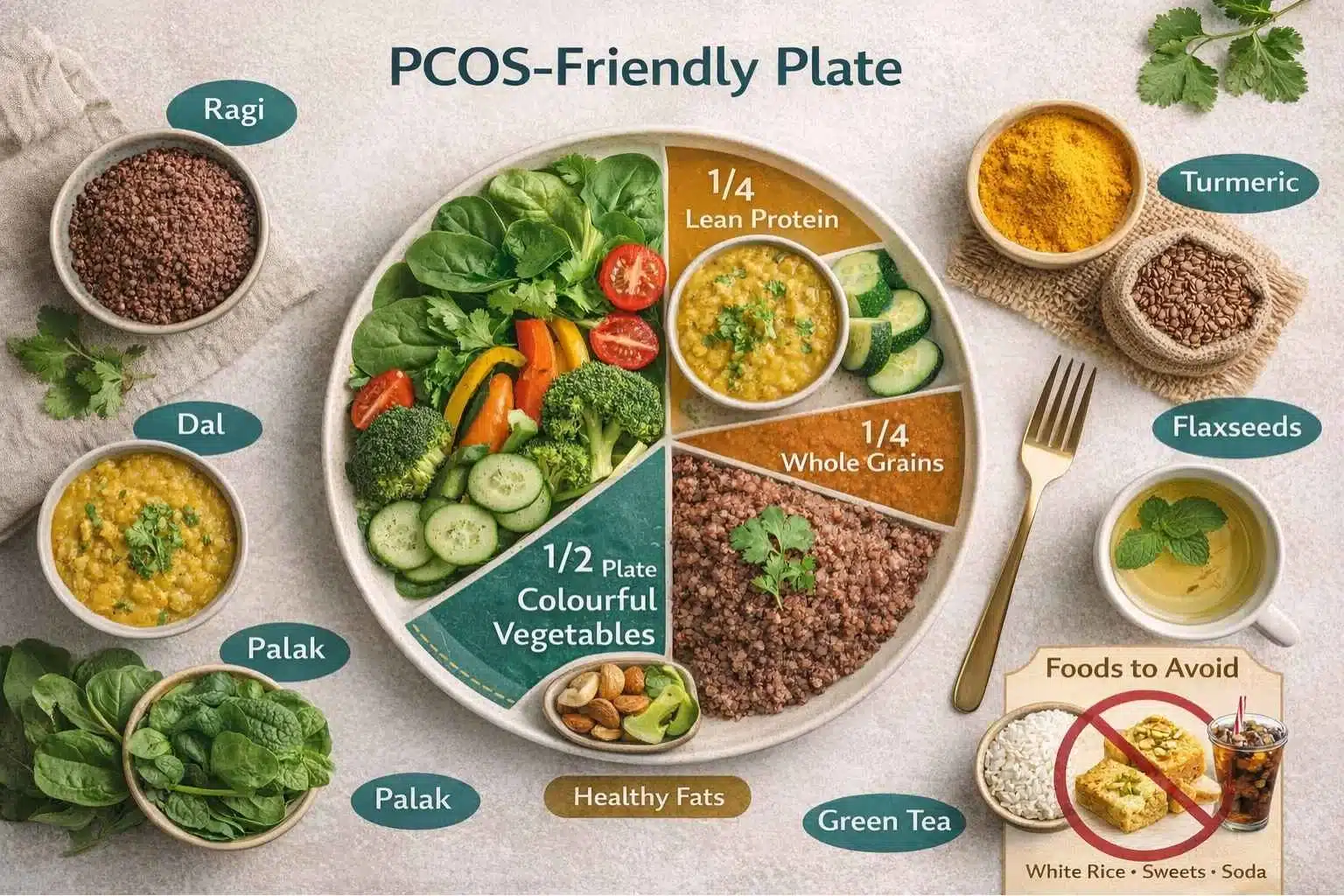
Foods to Include
Low-Glycemic Index (GI) foods: Whole grains (brown rice, oats, quinoa, ragi), legumes (lentils, chickpeas), and most vegetables help maintain stable blood sugar levels and reduce insulin spikes.
Lean proteins: Fish, chicken breast, eggs, paneer, and tofu support muscle mass and keep you feeling full longer.
Healthy fats: Nuts, seeds (especially flaxseeds and walnuts which contain omega-3s), avocado, and olive oil help reduce inflammation.
Anti-inflammatory foods: Turmeric, ginger, leafy greens (spinach, kale), berries, and green tea can help lower inflammation markers.
Foods to Limit or Avoid
Refined carbohydrates (white bread, white rice, maida), sugary drinks and sweets, processed and fried foods, excess dairy (some studies suggest dairy can worsen acne and hormonal issues), and excessive caffeine and alcohol.
Lifestyle Recommendations
Exercise: Aim for 30 minutes of moderate activity most days. A mix of cardio (walking, swimming, cycling) and strength training is ideal. Even a 30-minute daily walk can make a significant difference.
Stress management: Chronic stress elevates cortisol, which worsens insulin resistance. Practice yoga, meditation, deep breathing, or any relaxation technique that works for you.
Sleep: Aim for 7–8 hours of quality sleep. Poor sleep disrupts hormones that regulate appetite and insulin.
Can You Get Pregnant With Bilateral Polycystic Ovaries?
Yes, absolutely. This is perhaps the most important message — having bilateral polycystic ovaries does not mean you cannot have a baby. Research shows that women with PCOS ultimately give birth to just as many children as women without the condition. However, they may need more time and sometimes medical help to get there.
Here is how fertility is affected and what can be done:
The core issue is irregular or absent ovulation. If you do not ovulate regularly, there is no egg available for fertilisation. However, this does not mean you never ovulate — many women with bilateral polycystic ovaries still ovulate sporadically.
Steps to Improve Fertility
Lose weight if overweight: Even a 5% weight reduction can restore regular ovulation in many women.
Track ovulation: Use ovulation predictor kits, basal body temperature charting, or apps to identify your fertile window.
Ovulation-inducing medications: Letrozole is now considered the first-line treatment for ovulation induction in PCOS, with studies showing it leads to higher ovulation and live birth rates compared to clomiphene citrate.
Fertility treatments: IUI or IVF are options when simpler treatments do not succeed. At Arka Anugraha Hospital's Infertility Department, we offer comprehensive fertility support.
Treatment Cost for Bilateral Polycystic Ovaries in Bangalore
Understanding the cost of treatment helps you plan your healthcare journey. Here is an approximate breakdown of costs at hospitals in Bangalore (costs may vary based on the hospital, doctor, and complexity of the case):
| Treatment / Test | Approximate Cost (₹) |
|---|---|
| Gynaecologist Consultation | ₹500 – ₹1,500 |
| Pelvic Ultrasound (TVS / TAS) | ₹800 – ₹2,000 |
| Hormonal Blood Panel (LH, FSH, Testosterone, TSH) | ₹1,500 – ₹4,000 |
| Fasting Insulin + Glucose + HbA1c | ₹800 – ₹2,000 |
| Monthly Medications (OCPs / Metformin) | ₹300 – ₹1,500 |
| Ovulation Induction (per cycle) | ₹3,000 – ₹8,000 |
| IUI (per cycle) | ₹10,000 – ₹20,000 |
| Laparoscopic Ovarian Drilling | ₹50,000 – ₹1,00,000 |
| IVF (per cycle) | ₹1,00,000 – ₹2,50,000 |
Many health insurance plans in India now cover PCOS-related consultations, diagnostic tests, and medications. At Arka Anugraha Hospital, our team helps you with insurance paperwork and offers transparent pricing. Contact us for specific cost estimates.
Take the First Step Towards Better Health
Understanding bilateral polycystic ovaries is the first step. Our experienced gynaecologists at Arka Anugraha Hospital, JP Nagar, Bangalore are here to guide you with compassionate, personalised care.